This story was originally published at Georgia Health News.
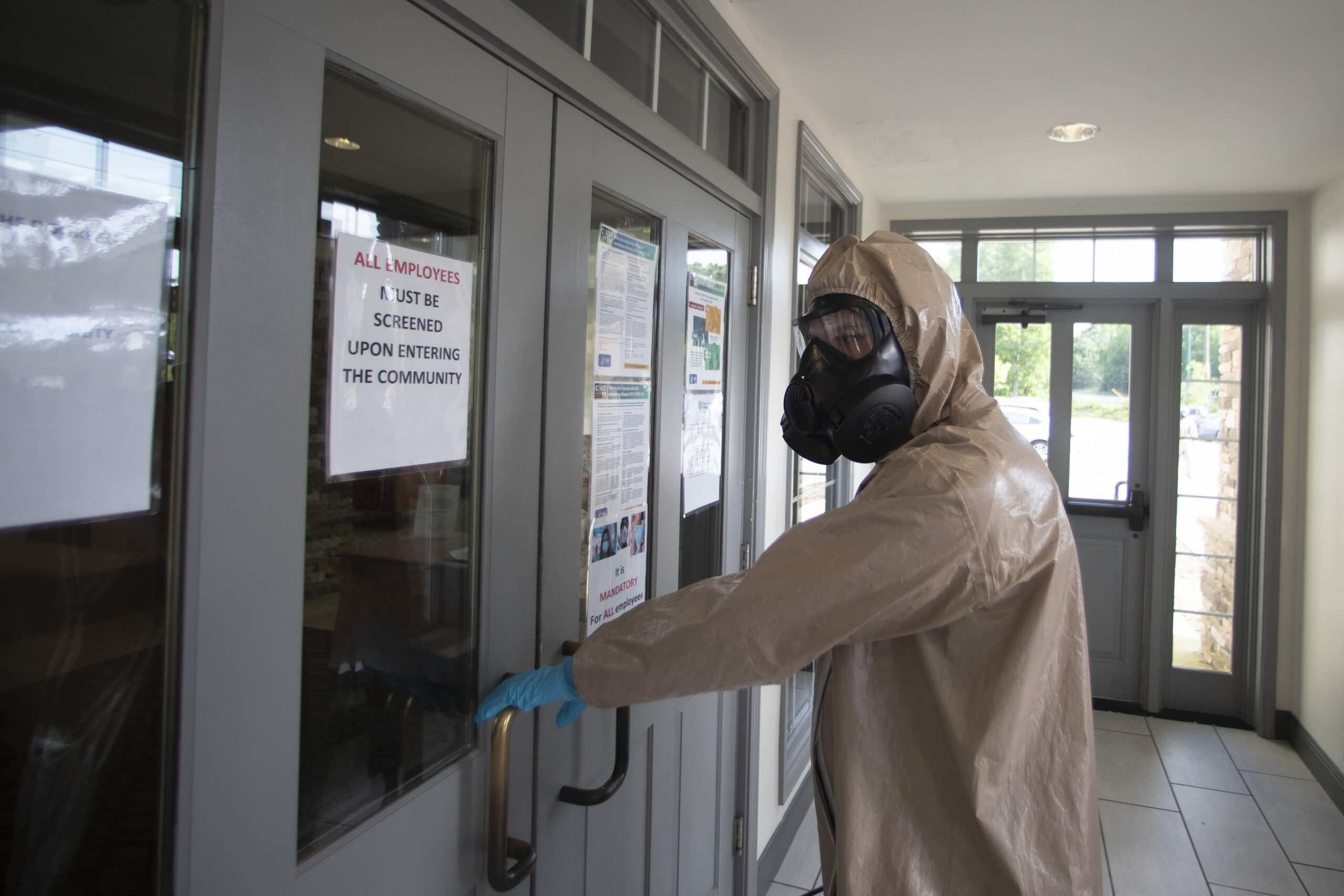
Nursing homes have become a constant battleground during the COVID-19 epidemic — in Georgia, around the nation and in several other countries.
Nearly half of Georgia’s 2,784 deaths have come from long-term care facilities, a percentage that’s mirrored in national statistics.
Read this story now for free
To continue reading, sign up for our newsletter and get unlimited access to WABE.org
You can select your preferences for news and local content. We will never share your email address. Learn how your newsletter sign-up will support WABE and Public Media








